
{kind=link}
Doctors’ Errors
In prior articles, I discussed several doctors who opined to varying degrees that children need not be vaccinated against COVID-19 (here, here, here, and here). Each of their arguments contained significant factual errors that undercut their argument.
- One doctor said that there is “about one in a million chance of death for a child under 19 from COVID”. This is false. In reality over 500 young people had died of the virus in the US when she made her claim, making her claim a mathematical impossibility that would require there to be over 500 million children in America.
- One doctor claimed that a vaccine trial for adolescents didn’t measure “clinical outcomes … because so few kids get sick with COVID-19.” This is false. In reality, the trial measured whether or not children got COVID-19, something that was in the title of the article. The vaccine worked. Sixteen children who received the placebo got the disease, while zero children who received the vaccine got the disease. The author apparently does not consider it a “clinical outcome” when a child gets COVID-19 in a trial of a vaccine designed to prevent them from getting COVID-19 and so didn’t mention this in his article.
- One doctor claimed that after “reviewing the medical literature and news reports, and in talking to pediatricians across the country, I am not aware of a single healthy child in the U.S. who has died of COVID-19 to date.” This is false. In reality, a simple Google search returns multiple news reports of otherwise healthy children dying of COVID-19 in the US, and a CDC study of 121 young people who died of COVID-19 found that 25% were healthy.
This is just a small sampling of the basic factual errors highly-credentialed doctors have made this pandemic.
Errors of Omission: The Virus
Making factual errors is one way to understate the harms caused by COVID-19. Another way is to not mention these harms at all. Some doctors haven’t made blatant factual errors, as their arguments not to vaccinate children are essentially devoid of any facts at all. If ten data points are needed to understand the risks and benefits of the vaccine, they cherry pick the three that support their position. For example, they rightfully cheered (here and here) when cases plummeted earlier this year, but are now silent as cases and hospitalizations rise to record levels in children.
Instead of providing concrete information about how the virus has harmed children, these doctors say only “the likelihood of severe outcomes or death associated with covid-19 infection is very low for children.” I wrote previously about why describing harms to children in this incomplete way is problematic. While I agree that children with COVID-19 have a low likelihood of severe outcomes and death, low likelihood events multiplied millions of times can add up to non-trivial numbers of very sick and dead children. People should know this. Yet, some doctors have written multiple articles on COVID-19 and children without simply even stating the number of hospitalized and deceased children. Some articles don’t even acknowledge that these tragedies can occur.
Errors of omission can be serious errors, and I try to avoid them. Though I strongly feel that adolescents should be vaccinated against COVID-19, I hope I’ve not shied away from presenting information that weakens this case. I’ve discussed the potential overcounting (and undercounting) of pediatric hospitalizations and deaths. I’ve discussed vaccine-myocarditis as evenly as I could and will discuss it every time I write about the vaccine. I’ve said previously (here and here) that a vaccine that sends young people to the hospital with heart inflammation should not be trivialized. Even if all affected individuals seem to recover back to normal after a short time, as pediatricians say they do, the possibility for long-term side effects is real and affected individuals will be advised to avoid vigorous activity for several months. Though I don’t do it perfectly, I try to be thorough, not to selectively present information to advance my beliefs. This doesn’t make me special. I’d think that any honest broker would do the same, especially when writing an article likely to be read by the general public.
The approach of trying to provide readers with all relevant information proved surprisingly controversial. One doctor defended his decision to omit harms of the virus in an article he wrote on vaccine-myocarditis by saying, “If you think *the virus* hasn’t had any airtime in the last 18 months then I’m not sure what more can be done for you.” Another doctor reacted similarly to my criticism by saying, “Failure to cite a widely reported statistic? Seems like a rather small nit to pick. I’m sure you can find more substantive arguments, no?” He also said that “[a] hallmark of novice science writers is starting every paper with a recitation of epidemiologic statistics which have been previously widely reported.” He felt doing so was a “waste of ink.”
While I agree statistics on COVID-19 and children are readily available, I don’t believe they are widely known. Do you know how many children have died of COVID-19, how many have been hospitalized, how many wind up in the ICU, or how many cases of MIS-C there have been? Do you know how just sick children with MIS-C often are? Do you know exactly how many children are contracting the virus and being hospitalized every day right now? Do you know that more children are being hospitalized now than ever before?
Maybe you do know these facts, but I’m sure the average person does not. I’m confident very few doctors know these all facts off the top of their head. Many people falsely believe that COVID-19 poses essentially no danger to children at all. This is precisely because basic facts have not been widely reported. Instead, numerous articles only report the harms to children as “rare” or falsely say that COVID-19 is less dangerous than the flu (it’s not). Of course, most scientific publications won’t be read by the general public, and it’s not necessary for every research paper to review all the numbers. However, opinion pieces published in medical journals are likely to be shared widely on social media and read by the general public. Doctors should not just assume that all readers will have all the facts at their fingertips. They should be cognizant of who may read their articles and what the effects of their omissions might be.
I generally believe that doctors who write about COVID-19 and children have an obligation to clearly inform their readers about the risk the virus poses relative to the vaccine, especially as this can be done in a couple of sentences. Dr. Aaron Carroll showed how easy this is to do. In an article advocating vaccinating children, he wrote,
At least 354 kids have died from COVID-19. Many more thousands have been hospitalized. More than 4,400 have been diagnosed with multisystem inflammatory syndrome in children (MIS-C), a “rare but serious condition associated with COVID-19,” and many more have been ill, even if they’ve recovered pretty well. Although COVID-19 has been nowhere near the danger that it has posed to adults and the elderly, it’s still been worse than most flu seasons for children.
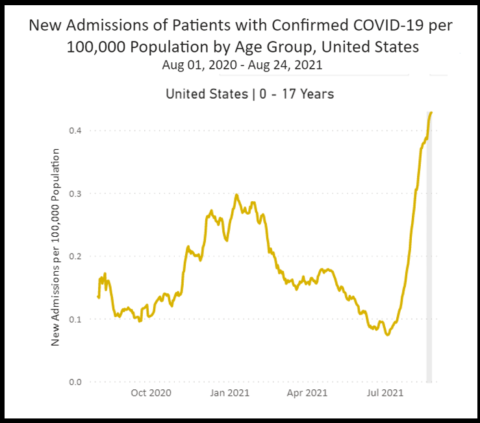
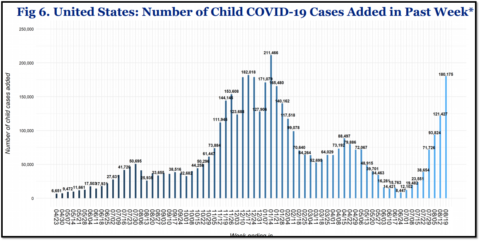
Combined with his acknowledgment of vaccine-myocarditis, these three sentences convey crucial information while using hardly any ink at all. (I’d only note that other tallies from the CDC and American Academy of Pediatrics report a slightly higher pediatric death toll). I’d bet that many people would not consider these harms “rare” when they are enumerated in this straightforward manner. I’d wager that more adolescents would be vaccinated if these numbers were widely known, especially given what the virus is doing to children right now. 180,000 children contracted the virus last week alone, the third worst week for children the entire pandemic. In Florida, children younger than 12 years have a 23% positivity rate and children ages 12 to 19 have a positivity rate of nearly 25%. An average of 321 children are being hospitalized with COVID-19 every day, the highest number thus far. 24 children died just last week, according to the American Academy of Pediatrics.
Recognition of past harms speaks to potential future harms and allows for informed policy discussions. Hundreds more children may die and many thousands more could be hospitalized if the virus is allowed to spread unchecked through the pediatric population, which is basically what is happening right now in many parts of the country. Perhaps this is one reason why some doctors who have expressed skepticism about the vaccine in children are habitually unwilling to simply present the facts about the virus. Acknowledging the reality of how COVID-19 has affected children drastically undermines their argument that they should not be vaccinated against it. As such, unwanted facts become unmentionable facts. It’s as if certain doctors have agreed on a collective code of silence, a form of contrarian omerta, where bad news must never be acknowledged. Ink conservation has nothing to do with it.
Perhaps another reason why some doctors are reluctant to acknowledge the reality of COVID-19 for children is they may feel obligated to say what they would do about it. I know that to varying degrees, these doctors are against masks, vaccines for children, vaccine mandates, and testing children in schools. However, other than wanting schools to be open, I’m not clear what they are for. I have no clue how they plan to keep children safe once they enter the classroom. Some doctors are calling for randomized controlled trials of masks and similar interventions. Doctors who say these interventions could “easily be studied” could actually do these studies. Then we’ll know what to do when schools open in 2022. However, these doctors’ plan for children today seems to be to cast doubt on measures to protect them, to never acknowledge unwanted news, and to repeat the mantra “severe illness in children is rare.” Unfortunately, saying this over and over again doesn’t help the hundreds of children who are going to the hospital every day with COVID-19. Evading reality is an easy way to evade responsibility.
Yet anyone who writes about COVID-19 and children has responsibility for their words. I basically agree with Dr. Nicholas Chrimes who said, “No one should be allowed to use the phrase ‘living with COVID’ without defining what that means in terms of acceptable rates of hospital admission & death.” Acknowledging reality doesn’t mean that policy positions automatically follow. Reasonable people may feel that schools should be open, but they should be honest about what the trade-offs will be. Again, hundreds of children could die and many thousands more could be hospitalized if the virus is allowed to spread unchecked through the pediatric population.
I’m glad schools will be open for my children in New York City. I’m really lucky my children are old enough to be vaccinated. New York City has decent overall vaccination rate, and it will use all the measures some doctors oppose to keep children safe. School employees are required to be vaccinated, children will wear masks, and they will be tested for the virus. I hopes that with these measures, COVID-19 will actually be as dangerous to children as the flu, which most of us previously felt was an “acceptable” rate of hospital admission and death. Nonetheless, some children will contract the virus at school. Some will get really sick and it’s possible some may die. I won’t sugarcoat this sad reality by merely describing the harms to children are “rare.” I also feel schools should be willing to reverse course if the virus spreads uncontrollably, which has already happened in multiple places where the situation is quite different from New York City. I don’t just want schools to open. I want them to stay open, and I want children to be safe. I am not sure if this is possible, but I’m certain that ignoring reality won’t help.
As Dr. Carroll showed, providing basic facts need not be alarmist. The overwhelming majority of children with COVID-19 will be just fine thankfully. It’s important to not forget this fortunate fact, which is why I’ve said exactly this every time I’ve written about this topic (here, here, here, and here). Even though everyone knows this, no one accused me of wasting ink for saying this. Similarly, no one accused me of wasting ink when I wrote just before the arrival of a nasty variant, “Barring a nasty variant, the worst is over for America and its children.” Even though it was common knowledge at the time, all of these doctors also used ink to share positive news about the virus. In fact all of them said the pandemic was essentially over or strongly implied it was ending (here, here, here, and here). Now that the pandemic has reached its most perilous moment for America children, ink preservation is suddenly a priority. This reveals an uncomfortable truth about the writers who insist on a rosier picture: ink is only considered “wasted” when it is used to share unwanted, inconvenient facts.
There are real-world consequences when prominent voices collectively omit information on how COVID-19 has harmed children, glossing over the harms by saying that COVID-19 is “a severe disease in adults, not in children.” One mother, whose unvaccinated 13-year-old daughter was hospitalized and intubated with COVID-19, said, “I just had a false sense of security that it was just like the flu and it wasn’t that serious. Obviously it is that serious and it was that serious. Now I can see.” It’s tragic that this mother had this false sense of security, though she was not alone. One doctor wrote on Twitter, “Admitted a child for Covid & the parent said ‘What? Kids get sick from Covid?’ Seemed sincerely shocked.” It is a clear failure of science communication that parents are still this misinformed this late into the pandemic.
Errors of Omission: The Vaccine
Though some doctors routinely omit negative information about the virus, they are only too eager to share negative information- and only negative information- about the vaccine. As is expected with those who are trying to convince people rather than inform them, long Twitter threads on vaccine-myocarditis make no mention of case series showing the condition has a very favorable short-term prognosis. While I fully agree that myocarditis in young people should not be minimized, the prognosis of these cases should not be hidden either.
Of the initial 323 cases identified by the CDC, 79% had no symptoms by the time they issued their first report, and all but 9 had been discharged from the hospital. Further cases series say:
- “All patients in this series had a benign course; none required intensive care unit admission” (Dionne et al)
- “Patients resolved their symptoms rapidly.” (Marshall et al)
- “Hospital course is mild with quick clinical recovery and excellent short-term outcomes” (Jain et al)
- “All patients received brief supportive care and were recovered or recovering at the time of this report.” (Montgomery et al)
- The clinical course of vaccine-associated myocarditis-like illness appears favorable, with resolution of symptoms in all patients.” (Rosner et al)
- “The clinical course was mild in all six patients.” (Mouch et al)
- “All patients had resolution of their chest pain, were discharged from the hospital in stable condition, and were alive with preserved left ventricular ejection fraction at last contact.” (Larson et al)
One of these articles concluded “Despite the risks of myocarditis associated with vaccination, the benefits of vaccination likely outweigh risks in children and adolescents,” which reflects the opinion of every major medical society with relevant expertise. Most countries with abundant vaccine supply are vaccinating adolescents. I have little doubt that if the myocarditis from the vaccine was as severe as the myocarditis from MIS-C, which can produce cardiac shock requiring ICU-care and life support, these doctors would readily share this information, which of course, would be appropriate.
Although all studies thus far are in agreement about the excellent short-term prognosis of vaccine-myocarditis, the frequency is a bit more uncertain. Data from Canada shows that it occurs in about 1 in 14,000 males age 12-17 years and 1 in 6,700 males age 18-24 years after the second dose. Data from Israel of people older than 16 years showed that there were 2.7 cases of myocarditis per 100,000 people and the average age was 25-years-old. The virus itself caused 11 cases of myocarditis per 100,000 people, as well as many other complications, of course. An FDA model based on “non-chart-confirmed cases from a US healthcare claims database” found the myocarditis rate to be potentially as high as 1 in 5,000 for boys age 16 and 17-years. Though I am unsure how reliable insurance claims are, it is similar to initial estimates from Israel, which reported a rate of 1 in 3,000-6,000 young males. (Israel reported that “95% are considered to be mild cases” and so decided to vaccinate all teenagers and high-risk younger children).
Even if the higher rate of vaccine-myocarditis turns out to be accurate, it is still lower than the risk of MIS-C, which occurs in about 1 in 3,200 children who contract the virus. Another study that reviewed electronic medical records, thus far not peer-reviewed, found that “Young males infected with the virus are up 6 times more likely to develop myocarditis as those who have received the vaccine.” Perhaps this is why I’ve read many articles about hospitals being overwhelmed with children with COVID-19, but I have yet to read an article about any hospital being deluged with teenagers with vaccine-myocarditis.
Doctors should aim to be comprehensive when sharing information about the vaccine, especially since multiple adolescents, including some with no underlying health issues, have died of COVID-19 after the vaccine was available to them (here, here, here, here, here, here, here, here, here, here, here, here, here, here, here, here, here, and here). In contrast, a review by the CDC found that zero children have died from the vaccine thus far. One mother, whose unvaccinated 18-year-old son ended up needing ECMO, said, “Seeing him like this, I think what if he got vaccinated? I don’t wish this on any mom.” She didn’t vaccinate her son saying, “I didn’t feel comfortable because you hear the good and the bad.” Again, it is a clear failure of science communication that parents are still this misinformed this late into the pandemic. Fortunately, enough voices are sharing the facts, and the vaccination rate in teens is increasing. Vaccination clinics are being held in honor of dead children, such as 17-year-old Schwanda Corprew who died four days before she was supposed to be vaccinated. Enterprising teens are even figuring out how to get vaccinated against the wishes of their parents.
It bears repeating, there are real-world consequences when prominent voices collectively omit information on how the virus has harmed children and how the vaccine can protect them. This is the central point of every article I’ve written here so far. It is never a “waste of ink” when doctors provide relevant, accurate information in articles likely to be read by the general public. Children older than 12-years shouldn’t be dying of COVID-19 or winding up on life support in the ICU today. These tragedies are completely preventable. Yet, they will continue to happen as long as people remain ignorant of a simple fact that some have inexplicably obscured: the virus is much more dangerous for children than the vaccine.
A flashback
If I didn’t have the facts at my fingertips, these doctors’ arguments to not vaccinate all eligible children might have been very compelling. However, I knew that over one in a million children died of COVID-19. I knew the vaccine trial measured whether or not children actually got COVID-19. I knew some healthy children had died of COVID-19. I knew the facts that others habitually omit. As such, I was easily able to spot the defects in these doctors’ arguments.
In doing this, I had a flashback to when I first became interested in the anti-vaccine movement many years ago. The first few times I read anti-vaccine articles, I found them plausible. I lacked the background knowledge to spot their flaws and was blissfully ignorant of the mendaciousness that characterizes the anti-vaccine movement. It was only when I dug further, often with the help Science Based Medicine, that I realized their grave flaws.
For example, in a collection of articles titled “200 Evidence Based Reasons NOT To Vaccinate,” Sayer Ji listed an article titled “A Measles Outbreak Was Reported in a Highly Vaccinated Population, San Diego, 2008.” Sounds bad, right? However, the full title of the article was “Measles Outbreak in a Highly Vaccinated Population, San Diego, 2008: Role of the Intentionally Undervaccinated.” The article concluded that “measles outbreaks can occur among clusters of intentionally undervaccinated children, at major cost to public health agencies, medical systems, and families.” In attempting to convince people vaccines didn’t work, Mr. Ji distorted the titles of articles that showed vaccines work quite well.
As a gullible naïf, this level of deception was astonishing to me. I knew moving forward that I needed to double check every “fact” I read in anti-vaccine articles. Usually these “facts” were blatantly false or crucial information was omitted. I have come to expect this from anti-vaxxers. I can now spot the errors and omissions in anti-vaccine articles from a mile away, and with Dorit Reiss, I wrote a book chapter about how to do this.
A realization
Before the pandemic, I didn’t feel the need to apply this level of scrutiny to articles written by a highly credentialed doctors at renowned medical schools. I believed such people made dedicated efforts to be both accurate and thorough. If they said a vaccine trial didn’t measure a clinical outcome or that no healthy children died from a particular virus, I wouldn’t rush to confirm this myself. I would assume the author had researched these claims and was accurately reporting their findings.
Now, as with anti-vaccine articles, I can no longer assume that some doctors accurately report basic facts or make a diligent effort to be thorough, including all relevant information. The errors and omissions I described previously are not isolated events in these doctors’ writing. Rather they are part of a consistent pattern where both the harms of the virus and the efficacy/safety of the vaccine are repeatedly minimized. Notably none of these doctors has made an error overestimating the dangers of the virus to my knowledge. All of their errors reinforce their prior belief that the virus isn’t that dangerous to children and the vaccine isn’t that great.
Unfortunately, these doctors continue to spread truly bizarre ideas in major newspapers and public forums.
- One doctor suggested that children who wear masks “can develop a mouth deformity and elongated face.” You can guess what the author thought about masks, even as the Delta variant is causing significant illness in children and shutting down schools everywhere.
- Another doctor thought the evidence-free claim that kids hospitalized with COVID-19 might really have RSV was a “super-interesting observation.” This “observation” is basically saying that the dire numbers and reports of frontline pediatricians can’t be trusted- COVID-19 isn’t really so bad after all. On a day when an average of 330 Americans were dying of COVID-19 and the trend was only going up, he tweeted “Crises?” with a graph showing that deaths are much lower than this winter. It is surprising that a doctor would ask whether hundreds of Americans dying a preventable death every day was a crisis, especially since he chastised those who called vaccine-myocarditis “mild.”
- Another doctor, who in June thought “that the US should suspend all vaccination in children under 18” due to vaccine-induced myocarditis, responded to the surge in pediatric hospitalizations by essentially trolling the American Academy of Pediatrics on Twitter for attempting to reassure parents that masks are safe. As pediatricians face harassments and threats for suggesting masks, he actually said, “there is no organization left in America that actually seeks to defend the interests of children.” He also said that institutions are failing American children because “many people hate Donald J Trump more than they love American children.” His own “plan” to protect children was that once “all adults are vaccinated their (children’s) risk of covid will decline precipitously.” When indeed cases fell earlier this year, this doctor accurately noted that “cases are FALLING PRECIPITOUSLY.” However, I have not seen him call much attention to the rise pediatric cases and hospitalizations to record levels.
- Another doctor said at the end of June that “children are not more susceptible to the delta variant, they’re threefold less likely to get any infection with any variant with any ancestral strain, and they’re half as likely to spread it.” The opposite of this is true, of course, and the Delta variant is affecting children more than ever before. She added,
It’s been a hard time, and people should have their summer. Delta variant, delta shmariant.”
You read that right, “Delta variant, delta shmariant.”
Reader beware
In my opinion, the egregiousness of these doctors’ errors, omissions, and statements mocking both the seriousness of the virus and organizations such as the American Academy of Pediatrics is not categorically different than the distortions of Mr. Ji, who truncated the title of an article to distort its findings. As with Mr. Ji, these doctors have made no obvious effort to correct their mistakes or fill in their omissions, even as the Delta variant causes increased harms to children.
Although they don’t treat children with COVID-19, they continue to have large platforms on TV, podcasts, YouTube, newspapers, and social media where they influence both public opinion and public policy. The have stellar academic credentials, speak with complete confidence, and unless you dig a little further, everything they say sounds very plausible. They are not obvious frauds, like Mr. Ji, who doesn’t even believe viruses make people sick. Certainly they are very hopeful, and hope makes us all feel better.
As a result of all this, these doctors are trusted and amplified by many influential people. Anti-vaxx propagandist Tucker Carlson repeated the false claim that no healthy American child has died of COVID-19 to millions of his viewers. Prominent politicians have made awful policy decisions based on the advice of Stanford doctors, and these politicians have parroted myths (here and here) they learned from doctors. A false claim that started on Twitter, with a doctor “just asking questions” about whether children with COVID-19 really have RSV, has the potential to influence policy for millions of children a few days later. Of course, these false claims always minimize the dangers of the virus to children and so children are paying the price.
I am unsure of the process by which these doctors made these errors and omissions. I believe in the principle of charity and believe there was no ill intent. These doctors are not supplement-selling grifters like Dr. Joe Mercola. Only one of them is selling anything, namely his books. I’ve written books too, and I highly recommend one of his books. I am sure they are excellent doctors in their respective specialties. They all have strongly encouraged adults to get vaccinated. They all want what’s best for children, and care deeply about the real harms of school closures and social isolation (which would improve if more teens were vaccinated), as well as the tragedy of global vaccine inequity.
One of them wrote an essay (with only blue-circle facts) titled “Kids don’t need Covid-19 vaccines to return to school” in February. In it he said, “The Covid-19 pandemic has harmed children — not because they have fallen ill from the virus, for the most part, but by the choices societies have made to protect adults who are vastly more likely to suffer from the disease.” I am sure he sincerely believes this is still true today, and the harms of school closures should not be glossed over. I’ve seen the harm in my own family. I have a real shy kid who had just made a few good friends when school shut down. They’ve only seen each other a few times since.
Moreover, it’s impossible to get everything right in the middle of a pandemic that seems to constantly shift in unpredictable ways. We are only human with biases and blind spots. I’ve caught errors in my articles only moments before a piece was published. I will make a mistake in one of these articles one day. I hope that you’ll assume I just goofed and that I wasn’t trying to mislead anyone. And please, if you spot an error or significant omission, tell me so I can issue a correction. I don’t want wrong or incomplete information being spread under my name. It matters how people react when others disagree with them. It’s not easy, but I try to follow the wisdom of Ralph Waldo Emerson who said, “Let me never fall into the vulgar mistake of dreaming that I am persecuted whenever I am contradicted.”
Though I am assuming good intent, I realize that I must approach a much wider set of writers with the skepticism that I formerly applied only to anti-vaxxers. I’m not saying these doctors are anti-vaxxers. I’m just saying they need to be fact-checked as if they were.